CONTEXT
The ongoing pandemic has led to a strategic shift towards a newly created ‘focal point’, constituting the need to train and equip the otherwise undervalued backbone of the global healthcare workforce – the frontline health workers [1]. It is imperative to point out that at the forefront of the efforts to contain the further spread of the novel coronavirus are a large number of healthcare workers that include not only doctors but a variety of cadres, who more often than not, are excluded from policy debates surrounding health policy in India. Consequently, the structural issues gripping the broad spectrum of healthcare workers – from nurses, lab technicians and pharmacists to ASHA workers, Anganwadi workers, ancillaries, among many others – often take a backseat. In this context, there is a felt need to highlight the structural issues faced by this section of India’s healthcare workforce, beyond the pandemic.
REGISTERED HEALTH WORKERS: NURSES AND MIDWIVES
India has around 8500 nursing institutes, which produce around 3 lakh nursing personnel every year [2]. The nursing cadre in India includes auxiliary nurse midwives (ANMs), general nursing midwives (GNMs), registered nurses (RNs), registered midwives (RMs) and registered lady health visitors (RLHVs) [3].
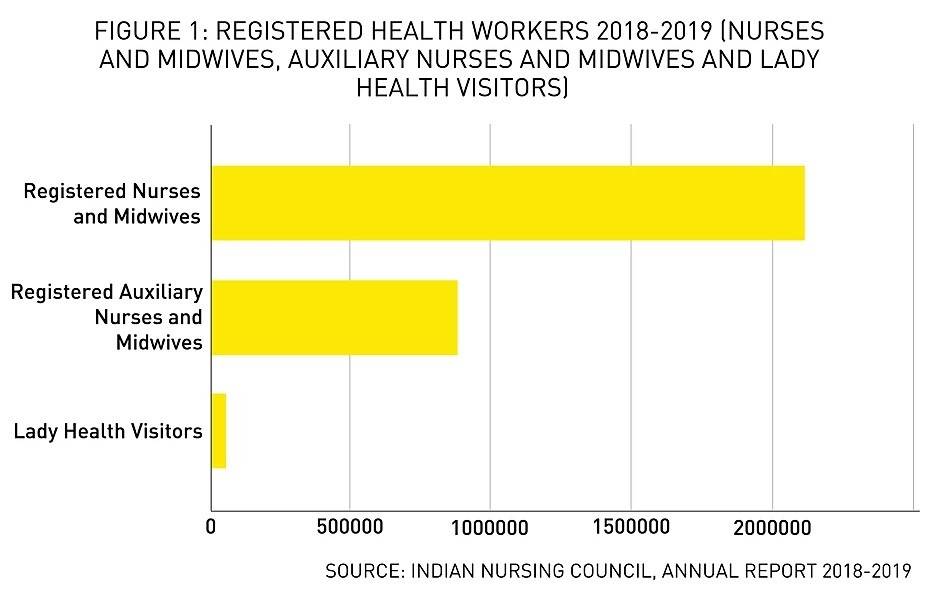
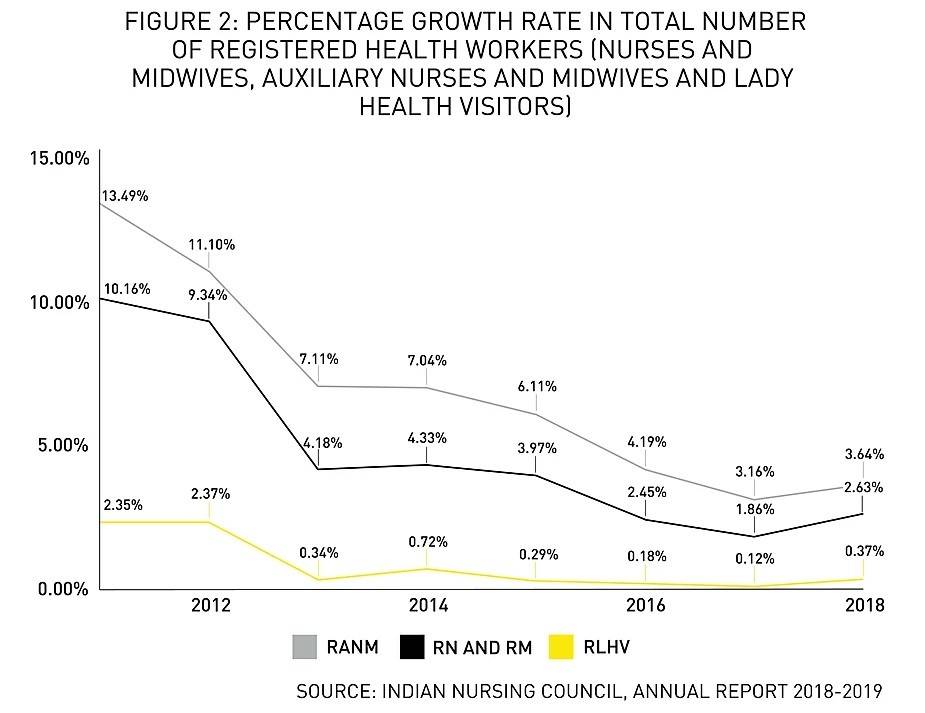
However, available nursing personnel constitute only 1.7 per thousand population, as opposed to 3 per thousand as recommended by WHO [4]. Between 2011 and 2018, there has been a steady decline in the year-wise growth percentage of each these sub-category of nurses- RANMs (10.16% to 2.63%); RNs and RMs (13.49% to 3.64%) and RLHVs (2.35% to 0.37%) [5].
This staggering decline in growth rates should be viewed in light of the poor status of medical qualification among nurses and midwives in India. According to a report published by WHO in 2016 (based on the 2001 Census), in India, merely 9.9% of active nurses and midwives were medically qualified, and only 22.2% held a graduate degree [6]. As of March 2019, out of the total seat share for all nursing programmes in India, only 22% of seats were allocated to B.Sc (Nursing), whereas P.C.B.Sc. (Nursing) and M.Sc (Nursing) constituted merely 9% and 7% of the total seat share respectively. Moreover, in 2015-16, the total number of enrolled students for B.Sc (Nursing) was 1,91,612, whereas the out-turn of students was only 46,563, about 24% [7].
It has been argued that with the launch of the National Rural Health Mission (NRHM), there has been an increase in employment opportunities for nurses in the public sector. However, most of these jobs are contractual, with meagre wages, poor working conditions and lack of job security. This had led to an increase in international migration among nurses, with India being the largest contributor to the global health force market and Indian nurses constituting 4.9% of the total nursing workforce in New Zealand and 3.3% of the same in Australia and the United Kingdom [8].
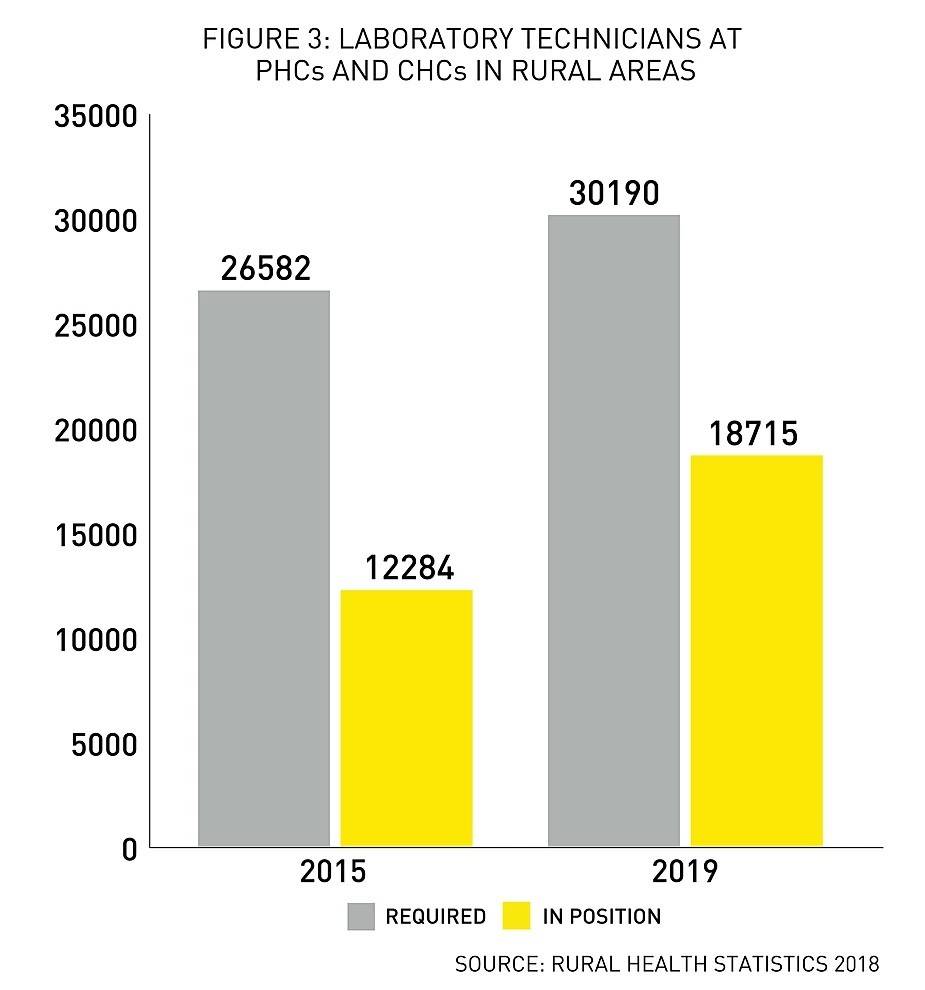
LABORATORY TECHNICIANS AND PHARMACISTS IN PRIMARY AND COMMUNITY HEALTH CENTRES (PHCs AND CHCs)
According to the Rural Health Statistics by the MoHFW, community health centres (CHCs) and primary health centres (PHCs) in rural areas have been facing a grave shortage of over 50% of laboratory technicians since 2005 [9]. In fact, as of March 31, 2015, 38% of the total PHCs in India were functioning without any laboratory technicians [10].
Likewise, presently, PHCs and CHCs in India are functioning with a prolonged lack of other paramedical staff such as pharmacists (25.11%) and radiographers (48%). There are merely 63 Health and Family Training Centres (HFWTC) and 67 Multipurpose Health Work Training Centres Male (MPW-M) in the country [11]. It has further been reported that along with technical infrastructure, many PHCs also lack adequate supply of water and electricity [12]. The neglect of public laboratory services stems from a limited understanding of PHCs as facilitators of preventive care. However, the availability of essential laboratory services for communicable and non-communicable disease, routine blood work, urine tests and pregnancy, among others are essential determinants in ensuring a timely and an efficient diagnostic process.
PRIMARY HEALTH CARE WORKERS: ANGANWADI WORKERS, ANGANWADI HELPERS AND ASHA WORKERS
In India there are 13,99,697, 12,82,847, 10,47,324 sanctioned Anganwadi Workers, Anganwadi Helpers and ASHA workers respectively [13] [14]. Yet, the work of these primary healthcare workers is categorised as ‘voluntary and honorary work’, and instead of a fixed salary, they are paid an honorarium (60% and 40% of the total honorarium paid by Central government and the respective states respectively). While ASHA workers receive a monthly honorarium of INR 2000 to INR 4000, varying from state to state, Anganwadi Helpers (AWHs) receive INR 1500 to INR 2,250 per month, and Anganwadi Workers (AWWs) at main Anganwadi Centres (AWCs) and mini-AWCs earn INR 3,000 to INR 4,500 per month and INR 1,500 to INR 2,250 respectively [15]. This is far below the minimum monthly wage in India, which is estimated at around INR 10,000 per month [16].
Since the work of primary health workers is considered to be voluntary, the honorarium does not include costs of travel and the amounts spent on buying stationery and other essentials, as well as additional expenses. Due to an inadequate honorarium and the absence of a fixed salary, these workers are forced to depend on monthly incentives, based on the type of services they render – from maximum remuneration of INR 5000 for administering anti-resistant drugs for tuberculosis to INR 1 for each packet of Oral Rehydration Solution (ORS) [17]. Despite the critical importance of these primary health workers and being an indispensable linkage between the community and health centres, they are still classified and recognised as sevika and sahayika and not karamchari. The lack of standardisation and inadequate regulation further obstructs the process of availing social security benefits such as Provident Fund, pension and Employees’ State Insurance (ESI), leading to a constant undermining of their skilled labour [18].
CONCLUSION
Despite the heavy reliance of over India’s growing population on community and primary health workers, skilled work performed by nurses, midwives, ASHA workers, Anganwadi workers and the supporting paramedical staff remains undervalued. Coupled with a heavy workload, poor working conditions, insufficient infrastructure and weak monetary incentives, there has also been a systematic devaluation of care work. Consequently, amidst a growing demand for primary healthcare facilities, India is also facing a severe crunch of healthcare workers.
It is also imperative to bring to fore the critical role played by ancillary and medical support personnel such as hospital attendants, canteen employees, ambulance drivers, cleaning and waste management workers, among many others in maintaining the equilibrium of the healthcare system. Yet, with an inadequate regulatory mechanism to safeguard the economic and social security of the ancillary personnel, this indispensable section of India’s workforce often finds itself outside the discourse surrounding healthcare in India. The ongoing pandemic has not only highlighted the necessity of trained and qualified doctors, but has also revealed the pressing need to address the structural and grassroots issues impacting the broad spectrum of healthcare workers in India for creating a robust healthcare system, beyond the pandemic.